


1Department of Dermatology, Zealand University Hospital, Faculty of Health and Medical Sciences, University of Copenhagen, Roskilde, 2Department of Clinical Immunology, Naestved Hospital, Naestved, 3Department of Clinical Immunology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, 4Department of Clinical Immunology, Aarhus University Hospital, Aarhus, 5Department of Clinical Immunology, Aalborg University Hospital, Aalborg, 6Department of Clinical Immunology, Odense University Hospital, Odense, 7Department of Epidemiology Research, Statens Serum Institut, 8Department of Haematology, Copenhagen University Hospital Rigshospitalet, 9Department of Neurology, Danish Headache Center, Copenhagen University Hospital and 10Novo Nordic Foundation Center for Protein Research, Copenhagen University, Copenhagen, Denmark
#These authors shared last authorship.
The risk factors and disease implications of hyperhidrosis are unknown. The objectives of this retrospective cohort study were to estimate the prevalence of hyperhidrosis and to compare demographic, lifestyle, and socioeconomic parameters in blood donors with and without self-reported or hospital-diagnosed hyperhidrosis. The study included blood donors from the Danish Blood Donor Study for the period 2010–2019. Registry data were collected from Statistics Denmark. Overall, 2,794 of 30,808 blood donors (9.07%; 95% confidence interval (95% CI) 8.75–9.40) had self- reported hyperhidrosis and 284 of 122,225 (0.23%; 95% CI 0.21–0.26) had hospital-diagnosed hyperhidrosis. Self-reported hyperhidrosis was associated with smoking (odds ratio (OR) 1.17; 95% CI 1.05–1.31), overweight (OR 1.72; 95% CI 1.58–1.87), “unemployed” (OR 1.60; 95% CI 1.24–2.08), “short education” (OR 0.76; 95% CI 0.64–0.90), and lower income (beta-coefficient –26,121; 95% CI –37,931, –14,311). Hospital-diagnosed hyperhidrosis did not differ from controls. Thus, self-reported hyperhidrosis was associated with potential hyperhidrosis risk factors (smoking, overweight) and disease implications (unemployment, low education level and income).
Key words: cohort studies; hyperhidrosis; overweight; smoking; socioeconomic factors.
Accepted Mar 17, 2021; Epub ahead of print Mar 18, 2021
Acta Derm Venereol 2021; 101: adv00435.
doi: 10.2340/00015555-3790
Corr: Mattias Henning, Department of Dermatology, Zealand University Hospital, Faculty of Health and Medical Sciences, University of Copenhagen, Sygehusvej 5, DK-4000 Roskilde, Denmark. E-mail: maahe@ regionsjaelland.dk
Hyperhidrosis is the medical term for too much sweating. It is not known if specific lifestyle habits increase the risk of sweating, or if sweating can negatively influence patients’ education and income. This study examined data for blood donors who had hyperhidrosis, diagnosed either in hospitals or by self-reported questionnaires. Additional data were collected on all participants from national registries and compared with data from blood donors without hyperhidrosis. Those with self-reported hyperhidrosis were more often overweight, smokers and had lower income and education than those without hyperhidrosis. Blood donors with hospital-diagnosed hyperhidrosis were not different from those without hyperhidrosis.
Hyperhidrosis (HH) is defined as pathologically increased sweat production that affects quality of life (1), which leaves a broad scope for interpretation. Thus, the prevalence of self-reported HH is 2–21% and the prevalence of hospital-diagnosed HH is 1–4% (1–11). Traditionally, HH is divided into primary and secondary HH. Primary HH manifests with excessive focal sweating, often from the armpits, face, palms, soles, trunk and groins/gluteal areas (12–14). The onset of primary HH occurs during childhood or puberty, and the aetiology remains unknown, although several studies have reported evidence to support a genetic link (13, 15). Secondary HH can manifest with general, regional and/or asymmetrical sweating and is related to cancer, endocrine-, infectious- and denervation diseases, as well as various medications (1, 5). Psychiatric illness is a well described co-morbidity to HH, but risk factors and disease implications of HH remain largely unknown (16). For demographic and lifestyle factors, only a few studies have reported correlations between HH and female sex and smoking (7, 17, 18). For socioeconomic outcomes, there is conflicting evidence suggesting that HH is associated with both reduced study and work ability, and with higher education and salary (19–21). The objectives of this study were therefore to estimate the prevalence of HH and to compare demographic, lifestyle, and socioeconomic parameters in individuals with and without self-reported or hospital-diagnosed HH.
Study design and setting
This is a retrospective cohort study within the Danish Blood Donor study (DBDS). The DBDS is a Danish nationwide biobank and cohort study on over 122,000 voluntary blood donors, aged 18–67 years, with a participation rate of 90–95% (22). Blood donors who provided a written informed consent and completed a DBDS questionnaire were considered eligible for study inclusion. There are 3 different editions of the DBDS questionnaire. The first edition was issued to blood donors upon blood donation between March 2010 and April 2015, the second edition was issued between May 2015 and May 2018 and the third edition was issued between June 2018 and March 2019. Each edition contained questions on demographics, lifestyles, and comorbidities. Some questions were included in all 3 editions of the DBDS questionnaire, such as smoking habits, while other questions were included in only 1 of the 3 editions, such as the HH screening question. Each blood donor could complete each questionnaire only once. With the unique Danish personal identification number, questionnaire data were cross-referenced with Danish national registers, as described below.
Hyperhidrosis cases
Individuals who donated blood in Denmark between June 2018 and March 2019 were asked to complete the third edition of the DBDS questionnaire, which included the HH screening question “Do you have troublesome sweating?” Those who answered “Yes, moderately” or “Yes, severely” were classified as participants with self-reported HH. Blood donors with diabetes or thyroid disease were excluded. Hospital-diagnosed HH was classified as blood donors who had completed at least one of the DBDS questionnaires between March 2010 and March 2019 and who had the International Classification of Diseased 10th revision (ICD-10) diagnosis R610 for localized HH. ICD-10 data were retrieved from the Danish National Patient Register, which contained diagnoses from all hospital inpatient and outpatient clinics for the period 1994–2019.
Control individuals
Blood donors who responded “No” in the HH screening question and who did not have an ICD-10 diagnoses for HH were classified as controls I. Controls II were blood donors who had completed at least 1 version of the DBDS questionnaire between March 2010 and March 2019 and who did not have ICD-10 diagnoses for HH (Table SI). Blood donors with diabetes and thyroid disease were excluded from controls I and II.
Thyroid disease and diabetes
Thyroid disease and diabetes were defined based on ICD-10 diagnoses and prescriptions (Table SI). Prescription data were obtained from the Prescription Database, which comprised all prescriptions for medications dispensed from Danish pharmacies in the period 1995–2019.
Demographics, lifestyle factors, and socioeconomic status
Questionnaire data on sex, age, height, weight, and smoking at DBDS inclusion was available for blood donors included between March 2010 and March 2019. Age was coded as a continuous variable and sex as a binary variable. Height and weight were used to calculate body mass index (BMI), and overweight was coded as a binary variable based on BMI ≥ 25 kg/m2. Smoking was coded as a binary variable indicating presence or absence of habitual smoking. Warm season was defined as inclusion in June, July, or August of 2018. Socioeconomic status (SES) was considered a nominal variable based on the main source of income and occupation during the year of inclusion. Data on SES was available from 1991 to 2018 and was divided in the following categories: “working”, “unemployed”, “on public support”, “studying”, and “pensioner”. “Working” was defined as employed, self-employed, or assisting spouse. “Unemployed” was defined as unemployed for 6 months within the last year or limited or no contact with the labour market with limited income from sickness benefits or leave benefits while not studying. “On public support” was defined as recipients of sickness benefits, education allowance for unemployed, and leave benefits. “Studying” was defined as blood donors who were studying. “Pensioner” was defined as blood donors who had retired from the workforce. “Education level” was defined as the highest achieved education at the time of inclusion. Data on education level covered the period 1981–2019 and was considered an ordinal variable, ranking ascendingly in the following order: “elementary school”, “high school”, “short education”, “medium education”, and “long education”. “Elementary school” was pre-school, primary school, or preparatory school. “High school” was general upper secondary education, vocational education, or qualification for entry to higher education. “Short education” was adult vocational training or short-cycle higher education. “Medium education” was medium-cycle higher education, undergraduate programs or bachelor’s degree. “Long education” was long cycle higher education. Income was defined as yearly personal salary, government transfers, and other incomes from interests and securities, in Danish krone, during the year of inclusion. It was coded as a continuous variable and data covered the period 1980–2018. Data on SES, education level, and income were collected from Statistics Denmark.
Statistical analysis
Histograms were used to determine normality. Continuous variables were reported as mean with standard deviation (SD) or median with interquartile range (IQR), depending on the distribution of data. Binary, nominal and ordinal data were presented as frequency distributions and percentages. Multivariable linear regression and multivariable logistic regression determined associations between HH status and overweight, smoking and, income. Multivariable nominal regression determined associations between HH and education level and SES. Regression analyses were adjusted for sex, age, overweight, smoking, and warm season, as they were potential confounders when coded as described in the Methods section (1, 7, 9, 17, 18). However, regression analyses with hospital-diagnosed HH was not adjusted for warm season, as the HH diagnosis was assigned to blood donors by hospital physicians and therefore not considered a potential confounder. The results of the regression analyses were presented in crude form and in adjusted form. The variable income was non-normally distributed and therefore box-cox transformed to find a suitable transformation and then analysed for association with HH. Effect sizes of associations were presented in odds ratio (OR) with 95% confidence intervals (95% CI) or beta-coefficients with 95% CI. Cases and controls with missing data were omitted from the statistical analyses. Model selection was based on Akaike Information criterion. Significance level was considered below 0.05. To correct for multiple testing, Bonferroni correction for 8 tests was applied to all p-values from regression analyses, which reduced the level of significance to below 0.00625. Whether p-values were significant after Bonferroni corrections is indicated in Tables I and II. Statistical analyses were conducted in R, version 3.6.3 (23–27). The assumptions of linear, logistic and nominal regression were met.
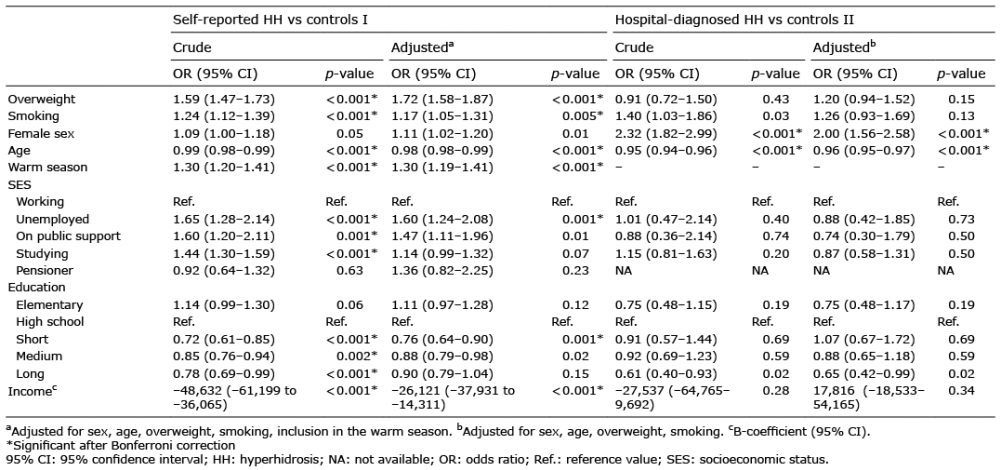
Table I. Logistic regression with hyperhidrosis as outcome, multinomial regression with socioeconomic status and education as outcomes, and linear regression with income as outcome
Table II. Logistic regression with hyperhidrosis as outcome, multinomial regression with socioeconomic status and education as outcomes, and linear regression with income as outcome
Ethics
Written consent was obtained from all included participants and the study was approved by the Central Danish Region Committee on Health Research Ethics (M-20090237 and SJ-740). The Danish Data Protection Agency approved the study (general approval number P-2019-99) in the Capital Region and Zealand Region data are handled under the same approval. All procedures were in accordance with the Declaration of Helsinki 1975, revised 1983.
Bias
Inclusion in the DBDS was based on convenience sampling. However, the inclusion was not based on presence of any disease, and therefore, this was a non-differential bias. In addition, inclusion was conducted by blood bank nurses who did not conduct any DBDS-related research, which further minimized the effect of this non-differential bias. Also, there was a risk of selection bias from only including healthy blood donors, which may hamper the extrapolation of results to other study populations. However, this bias was also non-differential because the DBDS inclusion was not based on any disease. The risk of confounding was generally low, as blood donors without severe disease or medication that could lead to HH were included. Furthermore, data were collected on potential confounders to adjust the statistical analyses.
Data sharing
Data from Danish registries are protected by the Danish Act on Processing of Personal Data and can only be accessed by application. Therefore, the research data for this study is not shared.
Fig. 1 shows a flow diagram for the study population. To summarize the responses to the HH screening question, overall, 2,902 of 30,808 blood donors answered that they had moderately or severely troublesome sweating, while 21,096 reported that they did not have troublesome sweating. In addition, 6,659 blood donors had mildly troublesome sweating and 151 answered that they did not know whether they had troublesome sweating. For results on demographics, see Table III.
Fig. 1. Study flow diagram of inclusion and exclusion of blood donors. DBDS: Danish Blood Donor Study; HH: hyperhidrosis; ICD-10: International Classification of Disease-10.
Table III. Demographics of self-reported hyperhidrosis, hospital-diagnosed hyperhidrosis (HH) and controls
Overall, 2,794 of 30,808 blood donors had moderate-to-severe self-reported HH, which implied a prevalence of 9.07% (95% confidence interval (95% CI) 8.75–9.40). In contrast, 284 of 122,225 blood donors had hospital-diagnosed HH, which equated to a prevalence of 0.23% (95% CI 0.21–0.26).
Self-reported HH was associated with overweight, smoking, reduced income, “unemployed” vs “working” and lower probability of “short education” vs “high school”. Hospital-diagnosed HH was not associated with any of the analysed parameters (Table I).
In a sub-analysis, the 284 blood donors with hospital-diagnosed HH were compared with the 2,746 blood donors with self-reported HH without a formal hospital diagnosis of HH. Hospital-diagnosed HH was associated with lower probability of overweight, “studying” compared with “working”, and higher income (Table II).
This retrospective cohort study found that the prevalence of self-reported HH in blood donors was in line with previous reports (3, 5–11). The prevalence of hospital-diagnosed HH was lower than previously reported (3, 4, 28). This may be the result of selection bias, as blood donors are implicitly healthy and have fewer diagnoses than the general population, or that individuals with hospital-diagnosed HH were receiving medications that precluded blood donation and thus study participation (29).
There are significant differences between the 2 groups. There were twice as many females as males with hospital-diagnosed HH, but near-equal proportion of females and males with self-reported HH. This suggests that HH occurs equally frequently in both sexes, but that women tend to consult physicians more readily for their HH symptoms.
This study also found a higher proportion of overweight among self-reported HH than among both controls and hospital-diagnosed HH. We speculate that extra body weight increases heat production, due to the increased physical burden or metabolic activity, or that the social stigma surrounding HH lead to an inactive lifestyle and weight gain. In the literature, few publications have shown higher BMI in individuals with self-reported HH (7, 11). Smoking is also known to elicit a sweat response, and the results indicate that participants with self-reported HH habitually smoked more often than controls (17, 30). Blood donors with self-reported HH, when compared with controls, were more often unemployed and had lower education and income, and also lower income than blood donors with hospital-diagnosed HH. Previously, it has been shown that individuals with HH experience a high degree of interference in studying and working ability from HH symptoms, as measured on the Dermatology Quality of Life Index (19, 21). Furthermore, the social isolation associated with HH may hamper academic attainment and the opportunity to enter better paid professions (19). However, blood donors with hospital-diagnosed HH did not differ from controls on SES, education level, or income.
We speculate that several factors contribute to the differences in prevalence, lifestyle habits, SES and income between self-reported and hospital-diagnosed HH. Firstly, low awareness of HH in the public, the stigma surrounding excessive sweating and seeking help for sweating, and the notion that treatments are futile lead to most adults with HH not seeking medical help for sweating (6, 31, 32). Next, lack of awareness of diagnostics and treatments for HH in physicians, and the seemingly benign symptomatology of HH, lead to many who seek help for HH not being given adequate treatment or referred to dermatologists (6, 32, 33). These factors result in the most resourceful individuals, who can overcome these obstacles, being most likely to eventually receive a HH diagnosis, which also can explain why individuals with hospital-diagnosed HH have healthier lifestyle habits and higher income. In addition, the common understanding that overweight and smoking can induce excessive sweating can explain why individuals who are overweight or smoke are under-represented in hospital-diagnosed HH, as these individuals may receive lifestyle interventions before a HH diagnosis (18, 30). This also suggests that the prevalence of hospital-diagnosed HH is, in general, underestimated.
Study strengths and weaknesses
Methodological strengths of the present study include a large database of healthy blood donors who did not have severe diseases that could lead to hyperhidrosis. In addition, access to important variables enabled adequate statistical adjustment that reduced the risk of confounding. In addition, all p-values were Bonferroni corrected to avoid type I errors.
Limitations include the study design that allowed for conclusions on associations only. The risk of misclassification was low, because we used physician-diagnosed HH or a self-reported HH definition, which was based on a previously validated diagnostic question (34). Other self-reported variables including smoking status, height and weight were simple questions that were unlikely to cause recall issues, and moreover, this probably affected HH cases and controls equally (i.e. on a non-differential bias). A further limitation is that individuals with other sweat-related diseases, such as bromhidrosis, can have been included in the group with self-reported HH and thus potentially influenced the results of this study. However, as the current study only included blood donors, none of these potential concurrent sweat diseases were severe or required chronic medication. Therefore, any potential concomitant sweat disease probably did not influence the results of this study (35). Likewise, psychiatric illness is associated with HH, and also with overweight, smoking, and low SES (16, 36, 37). As the study population consisted of blood donors who are not allowed to have psychiatric illness or receive psychiatric medication, any confounding from psychiatric illness was probably negligible (35). In addition, blood donors have a better health and lifestyle factors than the general population, which could limit the generalizability of the results (29). Likewise, we included adults between 18 and 67 years. Therefore, one should be cautious to extrapolate the results to age groups outside the study population, despite that it is well known that primary HH starts in childhood or adolescence and for some continues well beyond the age of retirement (12). The comparison of hospital-diagnosed HH and self-reported HH may introduce bias, as the latter is based only on subjectivity, and the former is based on subjective symptoms with or without objective findings. This also means that one should interpret differences between individuals with hospital-diagnosed and self-reported HH with caution. However, by current definition, HH is diagnosed based on subjective symptoms and does not require objective findings (13). The self-reported HH definition in this study was previously validated and we adjusted for several potential confounders that can influence the HH screening question response. Therefore, we consider that the subjectivity of self-reported HH does not invalidate the comparison with hospital-diagnosed HH.
Implications of the results
Blood donors with self-reported HH were most likely a mix of individuals with primary or secondary HH, because of the high prevalence of HH reported in this study, and because the study included blood donors who rarely have severe comorbidities that can cause secondary HH. This is supported by previous studies that have shown association between combined primary and secondary HH and both overweight and smoking (7, 17, 18). Thus, individuals who self-reported HH can potentially profit from primary prevention, i.e. weight loss and smoking cessation (38, 39). Another important primary intervention is to educate the public in HH so that more individuals with HH seek medical help. This is possible through working with HH patient associations. Another important strategy is to increase awareness of HH among primary healthcare physicians, which would lower the barrier to being diagnosed with HH. A possible solution to this is to publish HH research in general medicine journals. Secondary prevention, which focuses on interventions after development of HH, can potentially reduce the severity of HH symptoms. It is speculated that more comprehensive prevention strategies may decrease the subsequent risk of potential HH associated impairment, such as low SES, education level, and income. Additional data are, however, required to determine this. We also hypothesize that hospital-diagnosed HH was mainly primary HH, because we included individuals with localized HH, and donor selection excludes most sweat-inducing comorbidities (5, 35). This would also help explain why there was no association between hospital-diagnosed HH and lifestyle factors, as primary HH is thought to be primarily genetic (15). This is supported by previous research, which indicated a lack of associations between primary HH and smoking, overweight and employment status (7, 21, 40).
Conclusion
The prevalence of hospital-diagnosed HH is clearly lower than the prevalence of self-reported HH. Self-reported HH is associated with potential HH risk factors (i.e. smoking and overweight) and potential disease implications (i.e. unemployment, low education level and income). In contrast, hospital-diagnosed HH does not differ from controls on these parameters. We hypothesize that, in self-reported HH, a biopsychosocial disease model can explain the observed associations of this study. We further speculate that the most resourceful individuals, with superior coping mechanisms, are more likely to receive a diagnosis for their HH, which may also result in them achieving higher SES, education and income.
Karina Banasik (affiliation: Novo Nordisk Foundation Center for Protein Research, University of Copenhagen, Copenhagen, Denmark) is acknowledged for her work in the DBDS. The generous support of the Leo Foundation, Denmark (number LF 18002) is gratefully acknowledged.
Funding: MASH was provided a grant for research from Leo Foundation, Denmark (number LF 18002).
Conflicts of interest: MASH reports grants from Leo Foundation, Denmark (number LF 18002), during the conduct of the study. GBJ reports grants and personal fees from Abbvie, personal fees from Coloplast, personal fees from Chemocentryx, personal fees from LEO pharma, grants from LEO Foundation, grants from Afyx, personal fees from Incyte, grants and personal fees from InflaRx, grants from Janssen-Cilag, grants and personal fees from Novartis, grants and personal fees from UCB, grants from CSL Behring, grants from Regeneron, grants from Sanofi, personal fees from Kymera, and personal fees from VielaBio, outside the submitted work. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize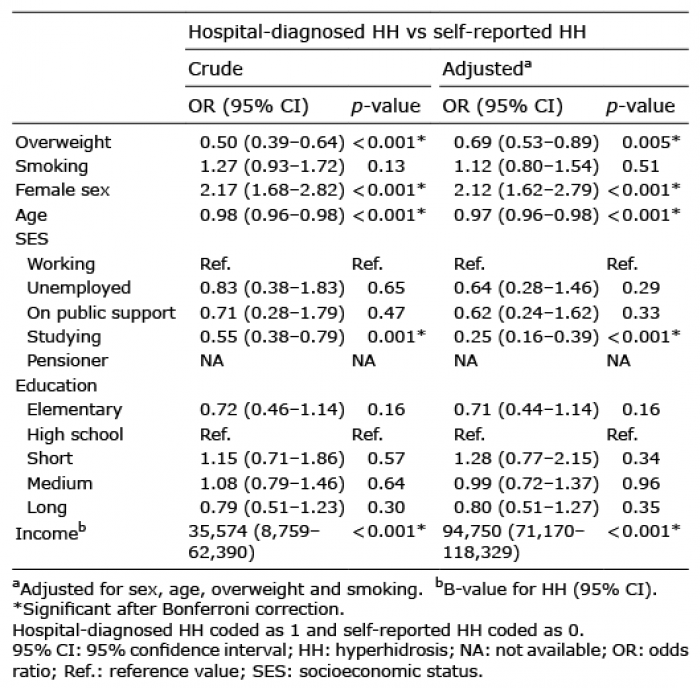 Click to show fullsize
Click to show fullsize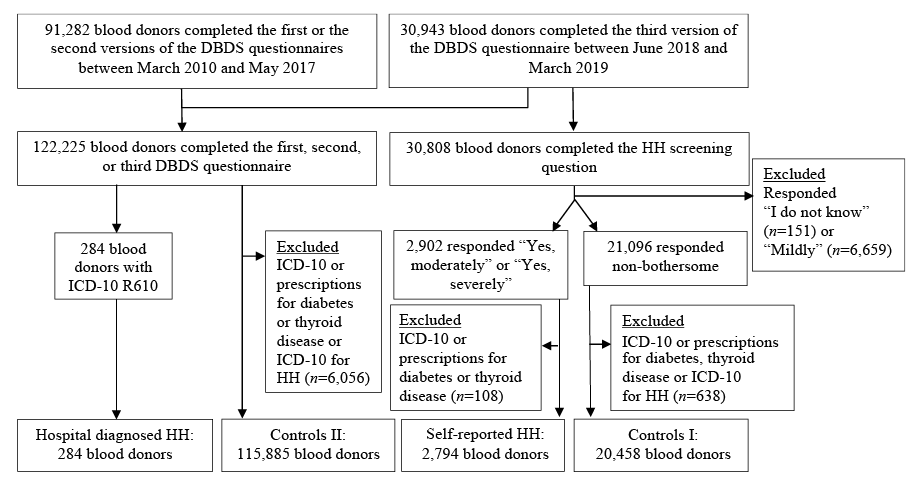 Click to show fullsize
Click to show fullsize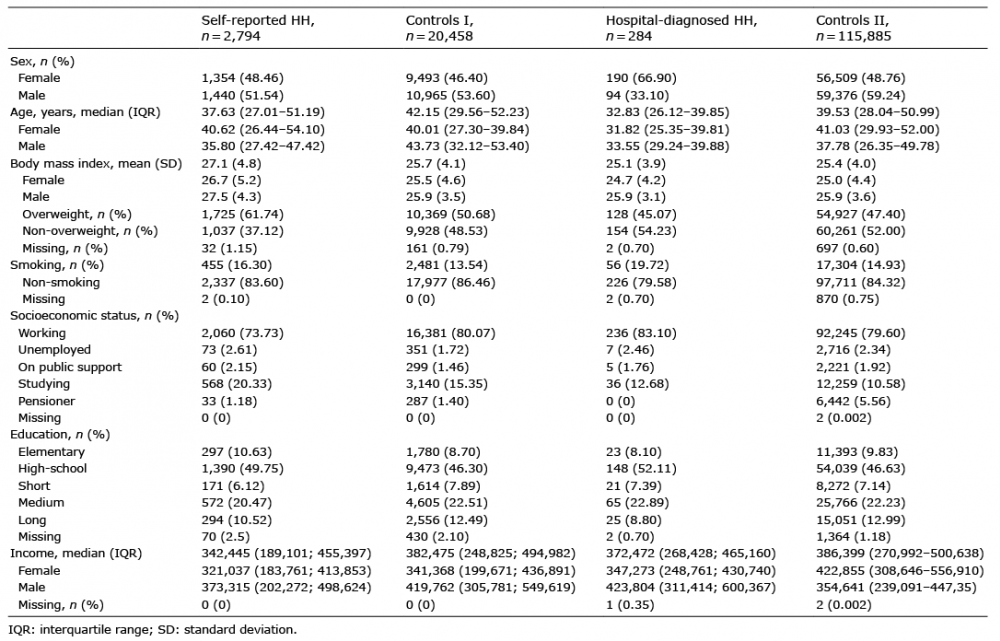 Click to show fullsize
Click to show fullsize